
What is an Anal Abscess or Fistula?
An anal abscess is an infected cavity filled with pus generally found near the anus and rectum.
Most of the abscesses are the result of acute infection in the internal anal glands of the anus.
An anal fistula( commonly called fistula in ano) is frequently the result of previous or current anal abscess. This occurs in upto 90 % of patients with abscesses. Fistula is a tunnel that connects a clogged gland inside the anal canal to the outside skin. A fistula can be present with or without an abscess.
Classification
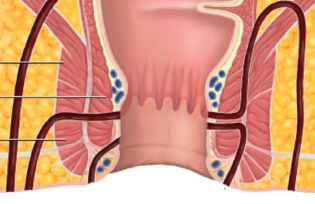
Anal abscesses are classified according to their location in relation to structures surrounding the anus and rectum( perianal, ischioanal, inetersphinteric, supralevator). Perianal is the commonest one and the supralevotor is the rarest one. If any of these abscesses spreads partially circumferentially around the anus and rectum, it is termed a horseshoe abscess.
Fistulas are classified by their realtionship to parts of the anal sphincter complex. Classified as intersphinctric, transphincteric, suprasphincteric, extrasphincteric. Intersphincteric is the commonest one and extrasphincteric is the rare one. These classifications are useful to make the treatment decisions.
- Superficial fistula
- Intersphincteric fistula
- Transphincteric fistula
- Suprasphincteric fistula
- Extra sphincteric fistula.
Symptoms
Anorectal pain, swelling, redness of the skin and fever are the most commonest symptoms.. occasionally rectal bleeding and difficulty in urination.
Pts with fistulas commonly have history of previous drained anal abscess, anorectal pain, drainage from the perianal skin, perianal itching can be presenting symptoms of fistula in ano.
Diagnostic studies
Most anal abscesses and fistula-in-ano are diagnosed and managed on the basis of clinical findings. Occasionally, additional studies can assist with the diagnosis or delineation of the fistula tunnel. Today, both traditional two-dimensional and three-dimensional endoanal ultrasound are a very effective manner of diagnosing a deep perirectal abscess, identifying a horseshoe extension of the abscess, and delineating the path of a fistula tract. This may be combined with hydrogen peroxide injection into the fistula tract (via the external opening) to increase accuracy. A pelvic MRI has been shown to have accuracy up to 90% for mapping the fistula tract and identifying internal openings.
Treatment of anal abscess
The treatment of an abscess is surgical drainage under most circumstances. An incision is made in the skin near the anus to drain the infection. This can be done in a doctor’s office with local anesthetic or in an operating room under deeper anesthesia. Hospitalization may be required for patients prone to more significant infections, such as diabetics or patients with decreased immunity.
Up to 50% of the time after an abscess has been drained, a tunnel (fistula) may persist, connecting the infected anal gland to the external skin. This typically will involve some type of drainage from the external opening. If the opening on the skin heals when a fistula is present, a recurrent abscess may develop. Until the fistula is eliminated, many patients will have recurring cycles of pain, swelling and drainage, with intervening periods of apparent healing.
Treatment of anal fistula
Currently there is no medical treatment available for this problem and the surgery is almost always necessary to cure an anal fistula. If the fistula is straight forward ( invoving minimal sphincter muscle), a fistulotomy may be performed. This procedure invoves unroofing the tract, there by connecting the internal opening with in the anal canal to the external opening and creating a groove that will heal from the inside out.
The surgery may be performed at the same time as drainage of an abscess, fistulotomy is a long standing treatment with high success rate in simple fistulas. But in high complex fistulas, chance of incontinenece is more, bcoz of involvement of more percentage of sphincter muscles. To avoid incontinence, in modern surgery there are other surgical options like coreout fistulectomy with primary repair, fibrin glue, endorectal advancement flap, vaaft, lift procedure etc.. in all these surgeries recurrence is almost 50 percent.
In this juncture ayurvedic ksharasutra therapy is having atmost important in treating all complex and simple fistulas.
About Ksharasutra Treatment
Ksharasutra Therapy is an Ayurvedic Parasurgical Technique. Great Indian Surgeon Sushruta narrated in his teachings the use of Kshara for cure of fistula in ano and other anorectal diseases. The work of Sushruta was later compiled as “Sushrut Samhita” in the 5th century A.D. Acharya Chakrapani Datta (10-11 Century A.D.) and Acharya Bhav Mishra (16-18 century A.D.) have described in their classical Ayurvedic texts, the method of preparation and treatment of fistula in ano by use of Kshara Sutra (K.S.). It is being used for the successful treatment of Anorectal Diseases from many years.
The presence of Kshar Sutra in the fistulous tract does not allow the cavity to close down from either ends and there is a continuous drainage of pus along the Kshar Sutra itself.
The Kshar Sutra slowly and gradually cuts through the fistulous tract from apex to the periphery. There is an ideal simultaneous cutting and healing of the tract and no pocket of pus is allowed to stay back.
The Kshara (Caustics) applied on the thread are anti-inflammatory, antislough agents and in addition, have property of chemical curetting. The Kshar Sutra remains in direct contact of the tract and therefore, it chemically curettes out the tract and sloughs out the epithelial lining, thereby allowing the fistulous tract to collapse and heal.
The Kshar Sutra, due to its antibacterial property, does not allow bacteria to multiply in its presence.
- Though the technique is effective in management of fistula in ano, the longer duration of treatment due to slow cutting and healing process makes the treatment difficult, especially in complex fistulas.
- Dr sarajas ayurveda anorectal hospital treats complex fistulas with modified kshara sutra treatments
- Fistulotomy+ ksharakarma( unroofing of the track till internal opening and application ayurvedic herbal caustic material)
- Advantage of the procedure is we can treat the fistula in very less time without any recurrence. Pt wound gets good fibrosis.
- Partial fistulotomy + ksharasutra(deroofing of the tract upto the sphincter complex and application of ksharasutra to the internal opening from the sphincter complex): we can implement this technique in straight transphincteric fistulas. Advantage of this technique is less duration, minimal incontinence and less recurrence.
- IFTAK( Interception of fistulous track and application of kshara sutra): In this technique interception of the proximal part of the fistulous tract is done at the level of external sphincter along with the application of kshara sutra from the site of interception to the infected anal crypt in the anal canal.
Indications
- High transphincteric fitula.
- Horse shoe type of fistula.
- Complex fistula with extension of tract upto scrotum, gluteus, thigh and abdomen.
- Intersphincteric fistula with supra levator extension.
- Fistula with supralevator extension.
- Blind internal fistulas with post anal abscess.